When you switch health plans, the biggest surprise isn’t always the monthly premium. It’s the bill for your daily medication. A $5 generic copay can suddenly become a $40 coinsurance charge - and you won’t know until you fill your prescription. This isn’t a glitch. It’s how formularies work. And if you don’t check them before switching, you could be paying thousands more each year.
What Exactly Is a Formulary?
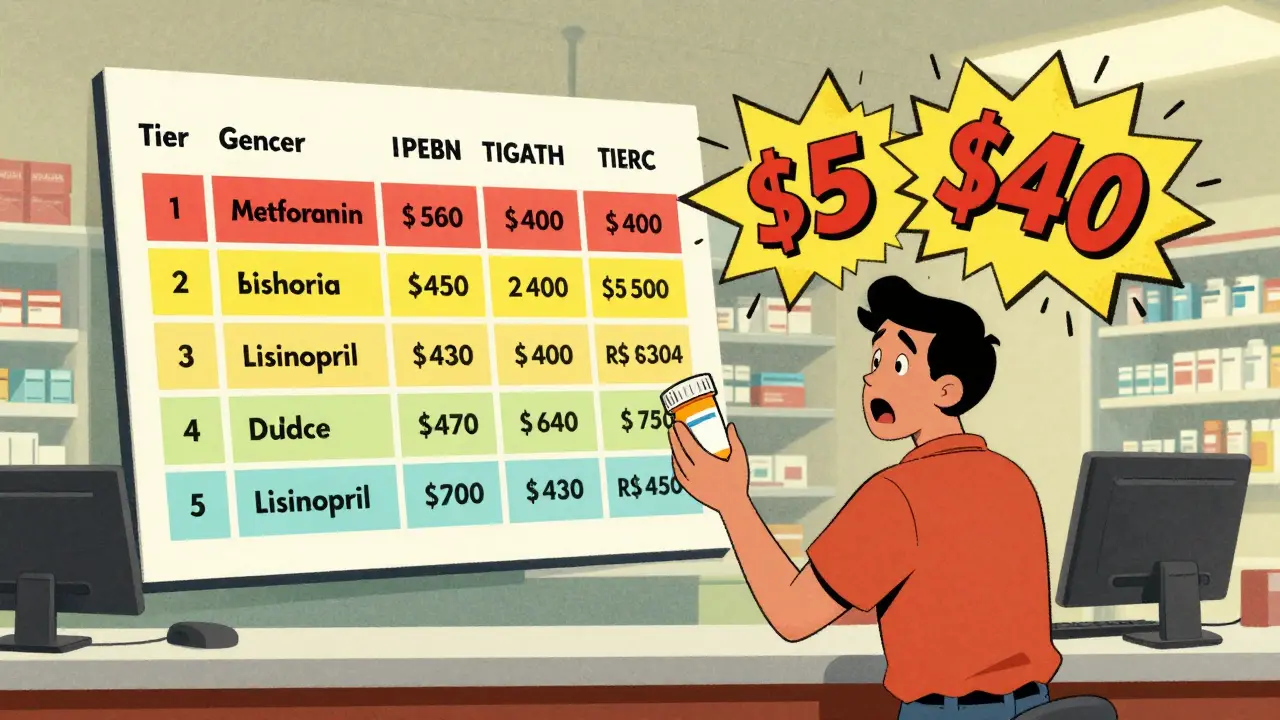
A formulary is just a list of drugs your plan covers. But it’s not as simple as “yes” or “no.” Most plans use tiers - like levels in a game - to decide how much you pay. Tier 1 is almost always generic drugs. These are the same as brand-name pills, just cheaper because the patent expired. They’re safe, effective, and often the first choice doctors make. But here’s the catch: not all generics are treated the same.Some plans put all generics in Tier 1 with a $3 copay. Others split them into Tier 1 (preferred) and Tier 2 (non-preferred). Why? Because different manufacturers make the same drug. Your plan might cover metformin made by Teva but not the one made by Mylan. Even though they work the same, your out-of-pocket cost could jump from $5 to $25. That’s not a mistake. That’s policy.
How Tiers Work Across Plans
Most health plans today use 3 to 5 tiers. Here’s what you’ll typically see:- Tier 1: Preferred generics. Copays range from $3 to $20. This is where most people should be.
- Tier 2: Non-preferred generics or brand-name drugs. Copays jump to $20-$50.
- Tier 3: Non-preferred brands or specialty generics. Coinsurance kicks in - you pay 20% to 40% of the cost.
- Tier 4/5: Specialty drugs. These can cost hundreds per month, even if they’re generic.
Medicare Part D plans often have 4 or 5 tiers. Marketplace plans (like those on Healthcare.gov) are required by law to use a 4-tier structure. Silver plans with Standardized Plan Design (SPD) are the most consumer-friendly: they waive your deductible for Tier 1 generics. That means you pay your $20 copay - no matter how much you’ve spent on medical care this year.
But not all plans do this. Some high-deductible plans (HDHPs) combine your medical and prescription deductible. So if your deductible is $3,000, you pay full price for every pill until you hit that number. For someone taking three daily generics, that could mean $1,200 in out-of-pocket costs before coverage even starts.
Why Your State Matters
Your location changes everything. California requires a separate $85 deductible for outpatient drugs - meaning you pay for prescriptions before insurance kicks in. New York, on the other hand, waives the deductible for generics and caps copays at $75 for specialty drugs. DC has a $350 drug deductible. Florida? No separate drug deductible at all.These rules aren’t random. States like California and New York passed laws to protect people on chronic medications. But if you move or switch plans without checking your state’s rules, you might assume your old plan’s benefits carry over. They don’t.
Cost Differences You Can’t Ignore
Let’s say you take three generics: metformin, lisinopril, and levothyroxine. In a Silver SPD plan, your annual cost is $240 ($20 x 12 months per drug). In a non-standardized plan with a $1,500 deductible, you pay full price until you hit that number. At $15 per pill, that’s $5,400 in drug costs before insurance helps. Even after the deductible, you might still pay 20% coinsurance - adding another $1,000.Medicare Advantage plans with drug coverage save users 18% on average compared to standalone Part D plans. But if you only take Tier 1 generics, the difference shrinks - because both types of plans often charge the same $0-$10 copay. The real savings come when you need more than just basics.
Employer plans vary wildly. Some charge $5 for generics before deductible. Others wait until you’ve paid $3,000 out of pocket. You can’t guess. You have to look.
What Most People Get Wrong
Here’s the truth: 68% of people switching plans don’t check if their exact generic version is covered. They assume “metformin” is metformin. But if your plan covers the 500mg tablet from Manufacturer A and your prescription is for the 1000mg from Manufacturer B, you might get bumped to Tier 2 - and your cost doubles.Another big mistake? Ignoring pharmacy networks. Your plan might say “$3 generic copay” - but only if you use a preferred pharmacy. Go to a non-preferred one? That same pill could cost $120. OptumRx data shows pharmacy network restrictions can raise generic costs by 300-400%.
And don’t forget mail-order. Some plans charge $0 for 90-day supplies via mail-order but $20 for 30-day retail refills. If you’re on three meds, that’s $720 saved a year.

How to Check Before You Switch
Follow this four-step process:- Get the full formulary. Don’t trust the summary. Download the complete list from the insurer’s website. Look for your exact drug names and manufacturers.
- Match your prescription. Check the strength (e.g., 500mg vs. 1000mg) and manufacturer. If your pill isn’t listed, assume it’s not covered.
- Check the pharmacy network. Use the plan’s tool to find your local pharmacy. Is it in-network? If not, how far do you have to drive?
- Run the numbers. Use the Medicare Plan Finder (for seniors) or Healthcare.gov’s plan selector. Plug in your meds. See what you’d pay annually.
CMS data shows people who complete all four steps reduce unexpected drug costs by 73%. That’s not luck. That’s strategy.
What’s Changing in 2025
The Inflation Reduction Act is changing the game. Starting in 2025, Medicare Part D will cap out-of-pocket drug spending at $2,000 a year. Insulin will stay capped at $35 per month. But here’s what’s new: generics will be split into Tier 1 (preferred) and Tier 1+ (non-preferred). That means even if you’re on generics, you could pay more if your plan decides your manufacturer isn’t “preferred.”More states are moving toward separate drug deductibles. California’s model is being studied by 12 other states. If you live in one of them, you’ll need to budget for drug costs separately from your medical bills.
AI tools like CMS’s new “Medicare Plan Scout” are making comparisons easier. In testing, they cut enrollment errors by 44%. Use them. They’re free.
Bottom Line: Don’t Skip This Step
Switching health plans isn’t just about premiums. It’s about what happens when you walk into the pharmacy. A $3 copay can turn into $40. A $0 monthly cost can become $1,200. And no one will warn you - unless you ask.If you take any daily medication - even just one - take 30 minutes before open enrollment. Download the formulary. Plug in your drugs. Compare the numbers. The difference between a good plan and a bad one isn’t the logo on your card. It’s what’s written on your prescription receipt.
Do all health plans cover generics the same way?
No. While all plans must cover generics, how they charge for them varies. Some have fixed $3-$20 copays. Others require you to meet a deductible first. Some split generics into preferred and non-preferred tiers. Medicare Advantage plans often have lower costs than standalone Part D plans, but only if your drugs are on their formulary.
Can I switch plans just to get better generic coverage?
Yes - during Open Enrollment (October 15-December 7 for Medicare, November-January for marketplace plans). You can switch based on drug coverage. But don’t wait until you need a refill. Check the formulary before you enroll. Once you’re locked in, you can’t change unless you qualify for a Special Enrollment Period.
What if my generic drug isn’t on the new plan’s formulary?
You have options. Ask your doctor if there’s a therapeutically equivalent drug on the formulary. You can also file an exception request - but approval isn’t guaranteed. Some plans offer temporary coverage while reviewing your request. If denied, you’ll pay full price or switch back.
Why does my generic cost more on a high-deductible plan?
Because high-deductible plans often combine medical and prescription deductibles. You pay full price for all drugs until you hit that deductible - which could be $3,000 or more. A Silver SPD plan waives the deductible for generics. If you take daily meds, avoid plans that don’t.
Is there a tool to compare drug costs between plans?
Yes. Medicare beneficiaries should use Medicare Plan Finder. Everyone else can use Healthcare.gov’s plan selector or insurer-specific tools like eHealthInsurance’s calculator. These tools let you enter your medications and see estimated annual costs. Use them - they’re accurate and free.

Kenzie Goode
February 25, 2026 AT 22:53Wow. I had no idea how much variation there was between plans. I switched last year and got hit with a $38 copay for metformin. Thought I was getting a better deal until I saw the receipt. This post should be mandatory reading before open enrollment.
Thanks for laying it out so clearly.
Dominic Punch
February 26, 2026 AT 03:32Let me break this down for you: it’s not about the drug. It’s about the manufacturer. Your plan doesn’t care if it works. They care if they got a better deal from Teva over Mylan. That’s corporate greed dressed up as ‘formulary management.’
And don’t get me started on pharmacy networks. I had to drive 45 minutes to a preferred pharmacy because my local CVS was ‘out of network.’ No one told me. No warning. Just a $117 bill for a $12 pill.
Check your formulary. Check your pharmacy. Check the damn manufacturer. And if you’re on Medicare, use the Plan Finder. It’s not hard. It’s just inconvenient for the insurers.
Valerie Letourneau
February 27, 2026 AT 02:40As a Canadian, I find this system both baffling and terrifying. We have universal drug coverage in our public system, but even our private top-ups are far more predictable. The idea that someone could be paying $5,400 for three generic pills before insurance kicks in… it’s not healthcare. It’s a lottery with your health as the prize.
I appreciate the clarity of your breakdown. It’s a service to anyone navigating this mess.
Khaya Street
February 27, 2026 AT 19:59Look, I don’t hate the system. I just hate how no one warns you. I switched plans because the premium was $20 lower. Thought I was saving. Turned out I paid $1,800 more in pills. My doctor didn’t know. My HR department didn’t know. I was on my own.
So yeah. Check the formulary. But also demand better transparency. This shouldn’t be a puzzle.
Brooke Exley
February 27, 2026 AT 21:57I’m a nurse. I’ve seen people cry in the pharmacy because they couldn’t afford their meds. One woman chose between insulin and her daughter’s school supplies. This isn’t policy. It’s cruelty disguised as cost control.
Yes, check the formulary. Yes, use the tools. But also fight for change. This system is broken. And the people who need help the most? They’re the ones getting buried under the fine print.
Lou Suito
February 28, 2026 AT 01:1268% don’t check? That’s not ignorance. That’s negligence. You can’t just assume. You can’t just hope. You have to verify. Every. Single. Time.
And don’t even get me started on mail-order. People think it’s a perk. It’s a trap. You can’t just switch to 90-day without checking refill windows. One delay and you’re off meds for two weeks. That’s not convenience. That’s risk.
Joseph Cantu
March 1, 2026 AT 19:19They’re lying. All of them. The insurers. The pharmacies. The government. They say ‘affordable generics.’ But the moment you need more than one, they turn it into a game of Russian roulette with your bank account.
I’ve been on levothyroxine for 12 years. Last year, my copay jumped from $4 to $42 because they switched manufacturers. No notice. No explanation. Just a bill. I called them. They said ‘it’s within policy.’
Policy? What policy? The one that lets them profit off your illness?
Lisandra Lautert
March 3, 2026 AT 03:28Formularies aren’t medical. They’re financial. And the tiers? They’re designed to confuse. You think you’re getting a ‘preferred’ generic. But if the tablet is 500mg instead of 1000mg? You’re bumped. No warning. No grace. Just a higher bill.
And don’t trust the ‘$3 copay’ ads. That’s a bait-and-switch. The real cost is hidden in the pharmacy network fine print. Always check the network. Always.
Cory L
March 4, 2026 AT 18:10I used to think generics were all the same. Then I got hit with a $27 copay for a drug that used to be $5. Turned out the new plan only covered the 500mg version. I was on 1000mg. So they slapped me with tier 2. I had to switch doctors just to get the right dosage written down.
Now I print out the formulary. I highlight my meds. I carry it to every appointment. It’s not fun. But it’s the only way to survive this system.
Sanjaykumar Rabari
March 5, 2026 AT 06:59Insurers are scam artists. They know you won’t read the fine print. They count on it. They don’t care if you can’t afford your medicine. They only care if you pay more. This isn’t healthcare. It’s a business. And you’re the product.
Bhaskar Anand
March 7, 2026 AT 02:21Why do Americans make everything so complicated? In India, generics are cheap because the government regulates prices. No tiers. No networks. No drama. Just affordable medicine. You want to fix this? Copy India. Stop overcomplicating it.
David McKie
March 7, 2026 AT 11:56Let’s be honest. This whole system is rigged. The formularies aren’t based on efficacy. They’re based on kickbacks. The manufacturers pay the insurers to put their version on Tier 1. The others? They get buried. And you? You pay more. Because you don’t know the difference.
It’s not a glitch. It’s a cartel.
Southern Indiana Paleontology Institute
March 8, 2026 AT 19:30Yall are overthinkin this. Just use Medicare Plan Finder. It tells you everything. No need to read 10 pages of fine print. Just enter your meds. Boom. Done. Why are you still making it hard? It’s 2025. The tools are right there. Use them. Or stop complaining.